



Sophie Pacek
Exercise Physiologist, Healthy Connections
As a child, my main sports were swimming, netball and tennis. Each activity requires high levels of shoulder mobility for strokes, throwing/shooting and hitting/serving. The shoulder joint is one of the most mobile in the body, but this can be at the expense of stability. Generally speaking, mobility and stability have an inverse relationship in joints – that is, if a joint is quite stable, it tends to be less mobile, and vice versa (Ehrman et al., 2013). For example, hinge joints like the elbow are very stable (i.e. hard (but not impossible) to dislocate) but can only move in one plane (bend and straighten) whilst the shoulder (a ball-and-socket joint) can flex, extend, abduct (raise out to the side), adduct and rotate but hence is less stable. The shoulder joint is more likely to dislocate if other tissues like ligaments, tendons and muscles are not as strong as they need to be. The major stabilising muscles of the shoulder girdle are collectively known as the rotator cuff, which will be our topic for this week’s blog!
The shoulder girdle
The shoulder girdle is the term given to the group of four joints around the shoulder (Ehrman et al., 2013).
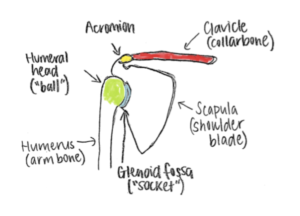
- The glenohumeral joint – what we would all know as the shoulder; it is the junction between the humerus (our upper arm bone) and the glenoid fossa of the scapula (shoulder blade). This is the ball-and-socket joint that allows us to move our arm in multiple directions.
- The acromioclavicular joint – this is a little joint you might be able to feel on the top point of each shoulder; it is the junction between the acromion of the scapula and our clavicle (collarbone). This is a gliding joint allowing more range of movement of the shoulder blade in relation to our ribcage.
The other two joints of the shoulder complex, the sternoclavicular and scapulothoracic joints, are less involved in the shoulder joint itself and more involved in the shoulder’s movement in relation to our ribcage. We are going to focus on the first joint (glenohumeral) in this blog.
The rotator cuff
I’m sure many of you would have heard of the rotator cuff, seeing as I come across many individuals at Healthy Connections who have tears in one or more of these muscles / tendons. Let’s take a closer look at each muscle.
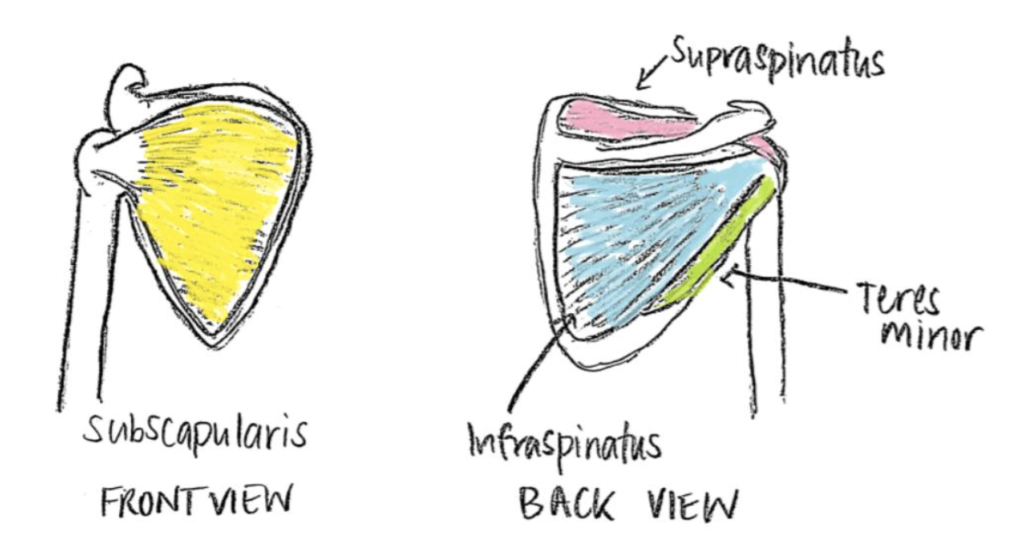
The rotator cuff is comprised of four muscles that form a cuff around the glenohumeral joint and are responsible for keeping the ‘ball’ (our humeral head) in its ‘socket’ (the glenoid fossa of the scapula). As the name suggests, these muscles aid in rotation of the ball within its socket, so we can perform daily activities like putting our hands behind our neck or reaching behind our back (‘doing up a ponytail’/’doing up a bra” movements) (Ehrman et al., 2013).
- Supraspinatus – aids in abduction (lifting arm up to the side)
- Infraspinatus – main contributor of shoulder external rotation (rotating arm outwards)
- Subscapularis – main contributor of shoulder internal rotation (rotating arm inwards)
- Teres minor – assists infraspinatus in external rotation and extension (carrying arm backwards)
Rotator cuff tendon injuries
One of the main rotator cuff injuries I deal with at Healthy Connections are tendon tears. The tendons of the rotator cuff run through the glenohumeral joint space and attach onto the ‘ball’ – this means that if the joint space is reduced, tendons can rub against the top of the scapula (especially when we have our arms above shoulder height). Tendon tears often occur over a long period due to repetitive shoulder movements or overuse. Due to the nature of tendons having limited blood supply, these tears often do not heal on their own; however, good function can be achieved without surgery.
What exercises should I do to improve my shoulder stability and mobility?
Shoulder rehabilitation exercises should aim to restore a certain level of function, strength, stability and range of movement. Stay tuned for next week’s blog where I will include specific exercises that will assist in achieving a balance between stability and mobility.
Until then, stay safe, wash your hands and keep moving!
Sophie
References
- Ehrman, J. K., Gordon, P. M., Visich, P. S., & Keteyian, S. J. (2013). Clinical Exercise Physiology. Human Kinetics: Champaign, IL.